

Abstract

While there has been significant increase in the number of older patients undergoing allogeneic hematopoietic cell transplantation (allo-HCT), the prevalence and the impact of geriatric syndromes associated with allo-HCT remains unknown. Using an institutional database and the electronic medical record, we retrospectively examined the incidence, predictive factors, and the impact of common geriatric syndromes of delirium, urinary incontinence, pressure ulcer, and mechanical fall among 527 patients age 60 and above (range 60-78.7) who underwent first allo-HCT for hematological malignancies at our institution from 2001 to 2016. We hypothesize that allo-HCT-associated geriatric syndromes negatively impact non-relapse mortality and overall survival.
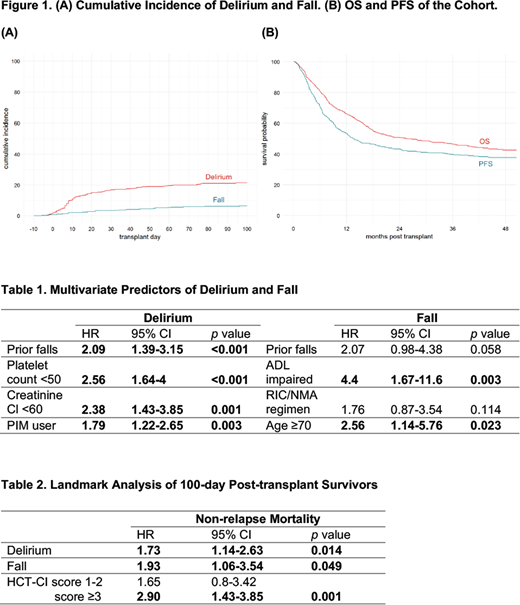
We identified all relevant geriatric events from the start of the conditioning regimen to 100 days post stem cell infusion. Among common geriatric syndromes, we found that delirium had the highest 100-day cumulative incidence at 21% (95% CI 18-25), followed by falls at 7% (95% CI 5-9) (Figure 1). There were only 11 incidences of new urinary incontinence and 3 incidences of new pressure ulcers. With a median follow-up of 46 months for survivors, the 3-year probability of overall survival and progression-free survival is 47% (95% CI 42-51) and 40% (95% CI 36-44), respectively (Figure 1). The 2-year cumulative incidence of non-relapse mortality is 28% (95% CI 24-32).
We assessed the association of standard, pre-transplant patient demographic, clinical, geriatric, and laboratory characteristics with the cumulative incidence of delirium and fall. We found that prior fall within last year, potentially inappropriate medications use prior to transplant admission (defined by 2015 American Geriatric Society updated Beers criteria), platelet count <50 k/µl, creatinine clearance <60 ml/min predicted delirium in the multivariate analysis. Age over 70 and impaired activities of daily living (ADL) predicted fall in the multivariate analysis with prior fall within last year close to be a significant variable (Table 1).
We next investigated the impact of delirium and fall on transplant outcomes. Delirium, but not fall, is independently associated with significantly increased risk of death at 100 days adjusted for standard transplant variables (OR 6.3, 95% CI 3-13.4, p<0.001). In addition, patients who experienced delirium and fall during their initial transplant admission had significantly increased length of stay (11 and 15 days longer, respectively, both p<0.001). In a landmark analysis of 100-day post-transplant survivors, both delirium and fall are associated with significantly increased long-term non-relapse mortality, with hematopoietic cell transplantation comorbidity index (HCT-CI) as an additional significant predictor (Table 2).
While limited by the retrospective design and likely under-reporting, our findings establish for the first time the baseline incidence and predictors of common geriatric syndromes associated with allo-HCT. Importantly, we have demonstrated significant negative impact of delirium and fall on the short- and long-term transplant-associated mortality and morbidities. The temporal pattern and impact of geriatric delirium and fall warrants preemptive, targeted, longitudinal, and multidisciplinary interventions to improve transplant outcomes and to expedite functional recovery after allo-HCT for older patients.
Perales:Takeda: Other: Personal fees; Novartis: Other: Personal fees; Abbvie: Other: Personal fees; Incyte: Membership on an entity's Board of Directors or advisory committees, Other: Personal fees and Clinical trial support; Merck: Other: Personal fees. Sauter:Juno Therapeutics: Consultancy, Research Funding; Sanofi-Genzyme: Consultancy, Research Funding; Spectrum Pharmaceuticals: Consultancy; Novartis: Consultancy; Precision Biosciences: Consultancy; Kite: Consultancy.
This icon denotes a clinically relevant abstract

